Appearance
Fertility & TRT
If you're considering TRT and might want children in the future, this is a critical chapter. TRT has major implications for fertility that you need to understand before starting.
The Reality
TRT suppresses sperm production in most men - but not always completely.
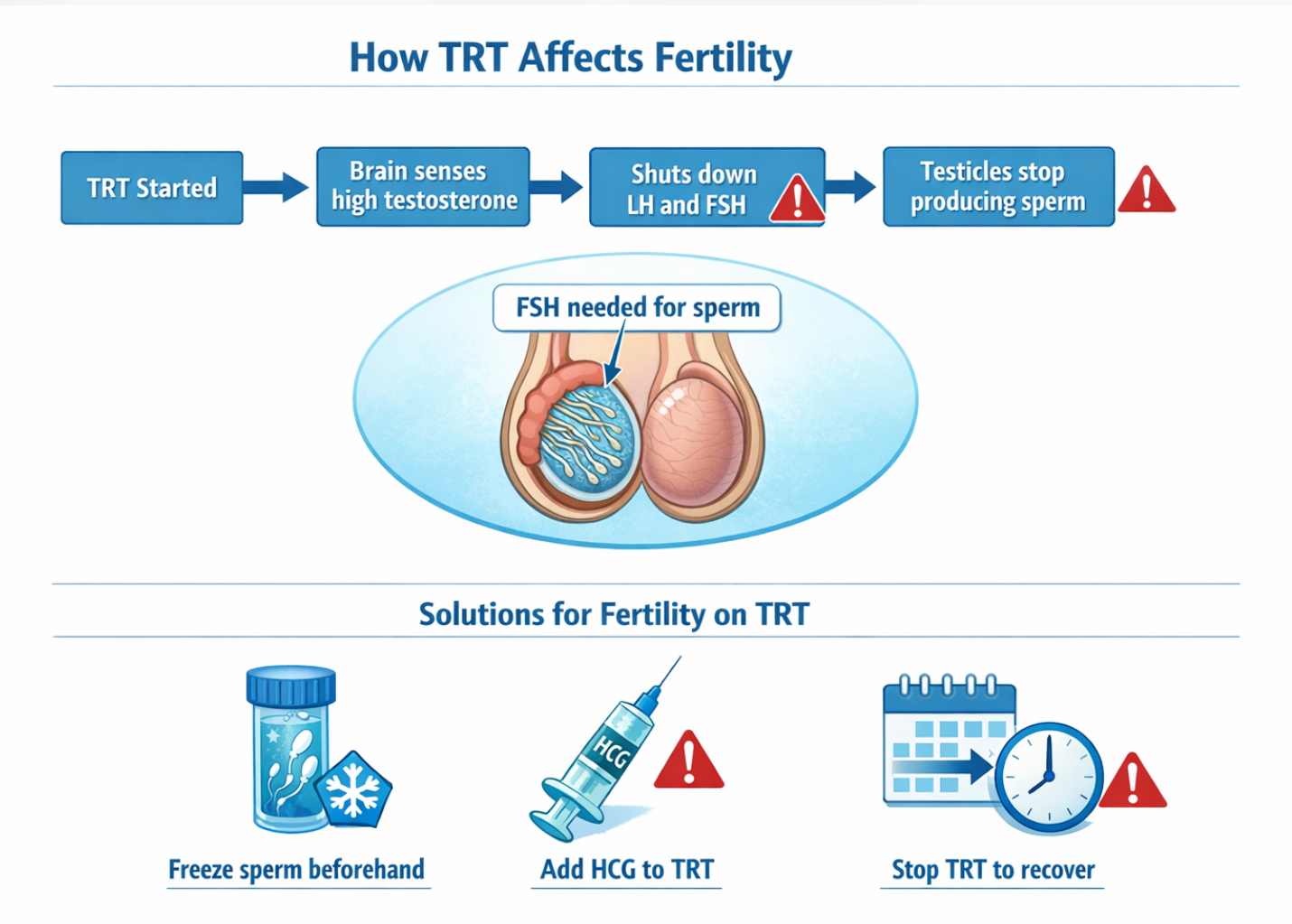
When you take exogenous testosterone, your body shuts down LH and FSH, which are needed for sperm production. Many men on TRT have severely reduced or zero sperm counts.
However, it's not universal. Studies show that roughly 10-20% of men on TRT maintain some fertility. Some men have even conceived children while on TRT. Don't count on it, but also don't assume you're completely sterile just because you're on TRT.
Why TRT Affects Fertility
Remember the HPG axis from Chapter 4?
When you inject testosterone:
- Your brain sees high testosterone → "We have enough!"
- Brain stops sending LH and FSH
- LH tells testicles to make testosterone → Now suppressed
- FSH tells testicles to make sperm → Also suppressed
- Sperm production dramatically decreases or stops
The intratesticular testosterone connection: Sperm production requires extremely high testosterone concentrations inside the testicles - about 50-100x higher than what's in your blood. When you inject testosterone, your blood levels are fine, but your testicles stop producing their own, so intratesticular testosterone crashes. This is why you can have great blood testosterone levels on TRT but still have no sperm - the local testicular environment has changed.
This is also why HCG helps preserve fertility: it stimulates the testicles to keep producing testosterone locally, maintaining that high intratesticular concentration that sperm need.
The Shrinkage Question
Yes, testicles often shrink on TRT.
Without the constant stimulation from LH, the Leydig cells (which make testosterone) and the seminiferous tubules (which make sperm) both atrophy.
Typical testicular changes on TRT:
- Shrinkage of 10-25% is common
- Some men notice little change; others notice significant
- Size often (but not always) returns if TRT is stopped
For many men, testicular shrinkage is more psychological than functional. Your testicles still exist; they're just smaller because they're not working as hard.
If this bothers you, HCG (discussed below) can prevent or minimize shrinkage.
Options for Fertility Preservation
If you want to preserve fertility while on TRT, or might want children later, here are your options:
Option 1: Freeze Sperm Before Starting TRT
This is the most reliable option.
Before starting TRT, go to a fertility clinic and bank your sperm. This provides a guaranteed backup regardless of what happens to your natural fertility.
Cost varies ($300-1000 for initial collection and storage, then annual storage fees), but it's worth considering if you're unsure about future family plans.
Option 2: Use HCG Alongside TRT
HCG (Human Chorionic Gonadotropin) can maintain testicular function and fertility while on TRT.
How HCG works:
HCG is structurally similar to LH (the hormone that tells testicles to work). When you inject HCG, your testicles think they're getting the LH signal, even though your pituitary has stopped producing it.
This keeps the testicles functioning, maintaining:
- Intratesticular testosterone (important for sperm production)
- Sperm production (at reduced but present levels)
- Testicular size
Typical HCG protocol with TRT:
- Dose: 250-500 IU, 2-3 times per week
- Injected subcutaneously (same as TRT SubQ)
- Started at same time as TRT or added later
HCG doesn't guarantee fertility on TRT, but it significantly improves the odds compared to TRT alone. Many men on TRT + HCG maintain measurable sperm counts.
If you might want children, adding HCG from the start is wise.
Option 3: Stop TRT When Trying to Conceive
If you're already on TRT without HCG, you can try stopping TRT to restore fertility. However:
Recovery is not guaranteed and takes time.
- It can take 6-12+ months for sperm production to recover
- Some men don't fully recover
- You'll feel terrible during recovery (low testosterone while waiting for restart)
- PCT (post-cycle therapy) can help but isn't magic
Option 4: Use HCG and/or FSH for Recovery
If you've been on TRT and want to restore fertility:
- Stop TRT (or reduce dose significantly)
- Add HCG (stimulates testosterone and some spermatogenesis)
- Possibly add FSH (recombinant FSH directly stimulates sperm production)
- Wait and monitor with semen analyses
Recovery timeline:
| Timeframe | What's Happening |
|---|---|
| Weeks 1-4 | LH and FSH starting to return |
| Months 1-3 | Testosterone production resuming |
| Months 3-6 | Sperm production restarting |
| Months 6-12 | Sperm counts potentially normalizing |
| 12+ months | If not recovered, may not recover |
HCG Monotherapy
Some men use HCG alone, without testosterone, as a treatment for hypogonadism. This can work in certain situations:
HCG monotherapy may be appropriate for:
- Men with secondary hypogonadism (the problem is the brain signal, not the testicles)
- Younger men wanting to preserve fertility
- Men wanting to "test" if their testicles can produce enough testosterone
How it works: HCG stimulates your testicles to produce their own testosterone. If your testicles are functional, testosterone levels rise.
Pros of HCG Monotherapy
- Preserves fertility (you're not adding external testosterone)
- Maintains testicular function and size
- Uses your own testosterone production
Cons of HCG Monotherapy
- Doesn't work for primary hypogonadism (testicles can't respond)
- Expensive (HCG costs more than testosterone)
- Requires 3x weekly or more frequent injections
- May not achieve levels as high as TRT
- Increases estradiol more than TRT (intratesticular testosterone gets extremely high, causing local estradiol production that leaks into blood)
HCG monotherapy works for some men, but many find they feel better on actual testosterone. The estradiol increase from HCG can be problematic, and the testosterone levels achieved are often not as robust.
It's worth trying if fertility preservation is paramount and you have secondary hypogonadism. But be prepared to switch to TRT + HCG if it doesn't work well for you.
Clomiphene for Fertility
Clomiphene (Clomid) and Enclomiphene are sometimes used to boost testosterone while preserving fertility.
How They Work
They block estrogen receptors in the brain, tricking the hypothalamus into thinking estrogen (and testosterone) is low. This increases GnRH → increases LH and FSH → increases natural testosterone AND sperm production.
The Problems
Clomid/Enclomiphene monotherapy has significant downsides:
- Decreased IGF-1: These drugs lower IGF-1 (insulin-like growth factor), which is important for tissue maintenance and recovery
- Eye issues: Some men develop visual disturbances (floaters, blurry vision)
- Mood effects: Some men experience emotional blunting or mood changes
- Not as effective long-term: Initial testosterone boost often diminishes over time
- Estradiol issues: The estrogen blocking can cause symptoms even though estradiol isn't actually low
Clomid can work short-term for:
- Young men with borderline testosterone wanting a boost
- Men trying to conceive who can't use TRT
- Diagnostic purposes (seeing if the HPG axis can respond)
But as a long-term monotherapy solution, it's often disappointing. Many men feel worse on Clomid than on actual testosterone, even if their numbers look better.
If you need it for fertility purposes short-term, fine. But don't expect it to be a long-term replacement for TRT.
Practical Fertility Strategy
Here's a practical decision tree:
| Situation | Recommended Approach |
|---|---|
| Definitely want kids, soon | Consider HCG monotherapy first, or delay TRT |
| Might want kids, not sure when | Freeze sperm, then TRT + HCG |
| Done having kids | TRT alone is fine |
| On TRT, now want kids | Add HCG, consider stopping TRT, see fertility specialist |
| Young man with secondary hypogonadism | Try HCG or Clomid first, preserve options |
Questions to Ask Yourself Before TRT
- Have I completed my family, or might I want children later?
- If I want children later, am I willing to freeze sperm now?
- Am I comfortable adding HCG to my protocol?
- Do I understand that recovery of fertility after TRT isn't guaranteed?
- Have I discussed fertility implications with my partner?
If fertility is important to you, discuss it with your doctor BEFORE starting TRT. Not after. The best time to preserve fertility is before you've potentially damaged it.
A fertility specialist (reproductive endocrinologist or urologist specializing in male fertility) can provide more specific guidance than a general TRT clinic.
Quick Recap
The Reality
- TRT suppresses or eliminates sperm production
- Testicles often shrink on TRT
- This is expected, not a rare side effect
Preservation Options
- Freeze sperm before starting (most reliable)
- Add HCG to maintain some testicular function
- Both are better than hoping for the best
Recovery
- Possible but not guaranteed
- Takes months to years
- HCG/FSH can help
HCG Monotherapy
- Works for some with secondary hypogonadism
- Preserves fertility better than TRT
- Often less effective at symptom relief
Clomid/Enclomiphene
- Short-term option for fertility preservation
- Long-term monotherapy usually disappointing
- Side effects limit usefulness
Next up: Estrogen Management - The much-misunderstood topic of estradiol, aromatase inhibitors, and why less intervention is usually better.