Appearance
The Hormone Control Center
Time to meet the boss. Your testicles produce testosterone, but they don't decide on their own how much to make. They take orders from headquarters: your brain.
Understanding this command structure is crucial because it explains:
- Why TRT shuts down natural production
- How fertility is affected
- Why certain medications work (or don't)
- The difference between types of hypogonadism
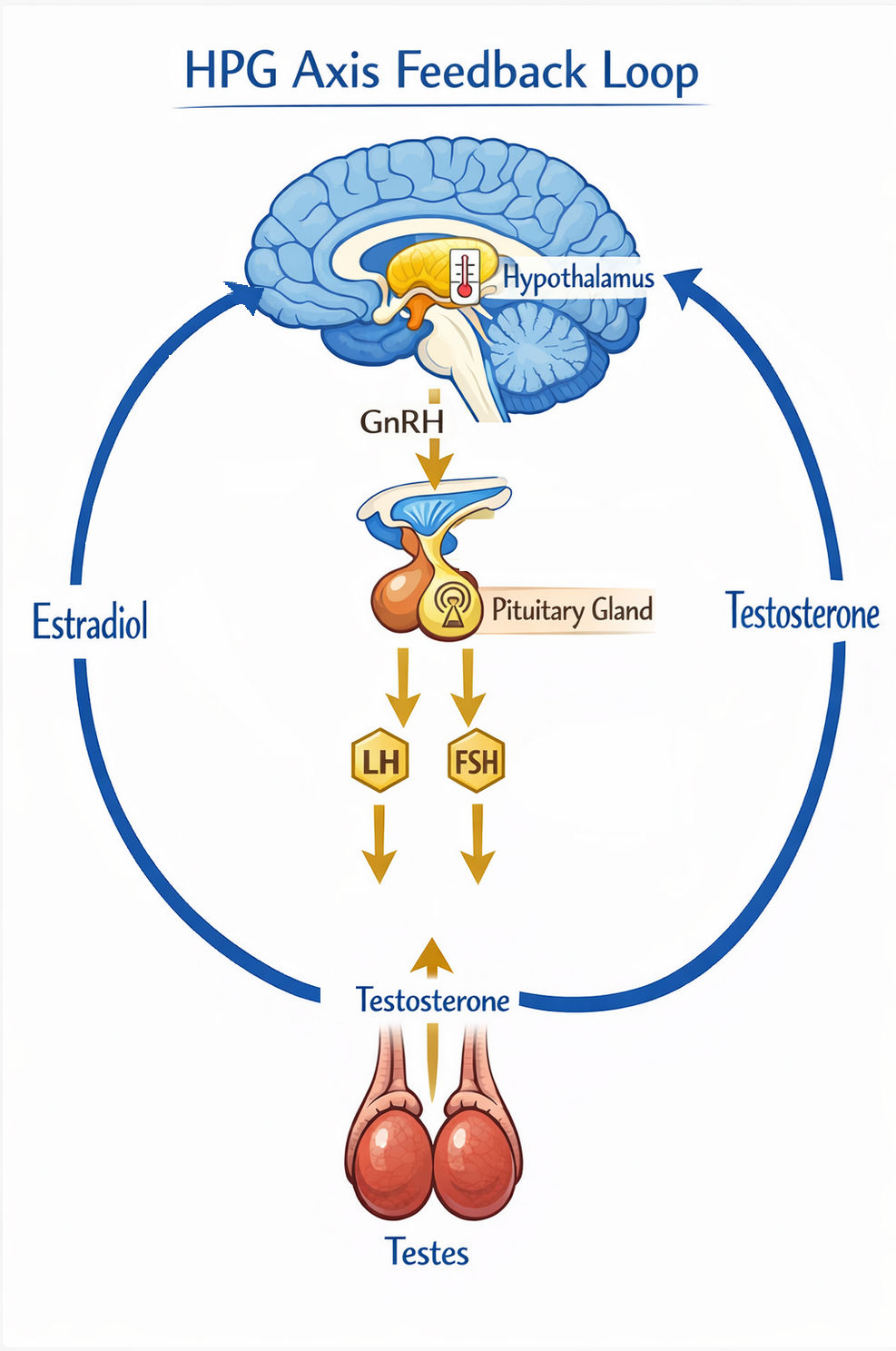
The HPG Axis: Your Body's Testosterone Thermostat
The system that controls testosterone production is called the Hypothalamic-Pituitary-Gonadal (HPG) Axis. Let's break it down.
Think of it like a thermostat system for your hormones:
- Hypothalamus = The thermostat itself (senses temperature, sets the target)
- Pituitary gland = The control box (sends the signal to turn on/off)
- Gonads (testicles) = The furnace (actually produces the heat/testosterone)
When the room (your blood) gets too cold (low testosterone), the thermostat (hypothalamus) notices and tells the control box (pituitary) to fire up the furnace (testicles). When it's warm enough, the system dials back.
The Chain of Command
Let's trace exactly how this works:
Step 1: The Hypothalamus
This small region at the base of your brain is the master regulator. It constantly monitors your hormone levels and decides if more testosterone is needed.
When it wants more testosterone, it releases a hormone called GnRH (Gonadotropin-Releasing Hormone) in pulses - not continuously, but in little bursts roughly every 1-2 hours.
Step 2: The Pituitary Gland
This pea-sized gland sits just below the hypothalamus. When it receives the GnRH signal, it responds by releasing two key hormones:
- LH (Luteinizing Hormone): Tells the testicles to produce testosterone
- FSH (Follicle-Stimulating Hormone): Tells the testicles to produce sperm
Step 3: The Testicles
When LH arrives at the testicles, special cells called Leydig cells get to work producing testosterone. FSH, meanwhile, works on the Sertoli cells to support sperm production.
LH and FSH are like two different work orders sent to the same factory.
LH says: "Make testosterone" → Leydig cells get to work
FSH says: "Make sperm" → Sertoli cells get to work
Both are needed for full testicular function.
The Feedback Loop
Here's where it gets clever. Your body doesn't want testosterone levels to go too high OR too low. So there's a built-in feedback system.
Negative Feedback
When testosterone levels rise, the hypothalamus and pituitary sense this and dial back their signals. Less GnRH means less LH, which means less testosterone production.
Back to our thermostat analogy: when the room reaches the desired temperature, the thermostat stops telling the furnace to run. If the temperature drops, it signals the furnace again.
This is "negative feedback" - high levels of the end product (testosterone) negatively affect the production signal.
The Estradiol Plot Twist
Here's something crucial that many people don't realize:
Estradiol (the main estrogen in men) is actually the PRIMARY negative feedback signal in the brain - even more so than testosterone itself in many ways.
Your brain has estrogen receptors that are very sensitive to estradiol levels. When estradiol goes up, it strongly suppresses GnRH and LH release.
This is why overweight men often have low testosterone: their extra body fat converts more testosterone to estradiol, which then tells the brain to shut down testosterone production. It's a vicious cycle.
Types of Hypogonadism
When testosterone is low, the question is: where is the problem? This matters a lot for treatment.
Primary Hypogonadism
The testicles themselves aren't working properly.
The brain is sending signals (LH is high, trying to stimulate production), but the testicles can't respond adequately. This can be due to:
- Genetic conditions (like Klinefelter syndrome)
- Injury or surgery affecting the testicles
- Infections (like mumps affecting the testicles)
- Chemotherapy or radiation
- Leydig cell changes (though many healthy older men maintain good function)
Lab pattern for Primary Hypogonadism:
- Testosterone: LOW
- LH: HIGH (brain is screaming for more)
- FSH: HIGH
Secondary Hypogonadism
The brain isn't sending proper signals.
The testicles could work fine, but they're not getting orders. LH and FSH are low or inappropriate for the low testosterone level. Causes include:
- Pituitary tumors or damage
- Obesity
- Certain medications (opioids, steroids)
- Excessive stress
- Sleep disorders
- Kallmann syndrome or other genetic conditions
- Head trauma affecting the pituitary
Lab pattern for Secondary Hypogonadism:
- Testosterone: LOW
- LH: LOW or inappropriately normal (brain is silent)
- FSH: LOW or inappropriately normal
If you have secondary hypogonadism, it's often worth investigating why before jumping to TRT. Sometimes fixing the underlying issue (losing weight, treating sleep apnea, stopping opioids) can restore natural production.
This is also where treatments like Clomid or HCG can work - they stimulate the system to produce its own testosterone. More on these in later chapters.
Mixed Hypogonadism
Sometimes it's both. The brain signal is weaker AND the testicles are less responsive. This can occur at various ages, often associated with accumulated health issues rather than age alone.
Testing the HPG Axis
Understanding this system explains why certain tests are important:
- Total Testosterone - What are your levels?
- LH - Is your brain sending the signal?
- FSH - Is your brain supporting sperm production?
- Estradiol - Is excess estrogen suppressing the system?
- Prolactin - High levels can suppress LH (pituitary tumor marker)
If testosterone is low and LH is also low, your doctor should investigate the pituitary gland. Sometimes an MRI is warranted to rule out a pituitary adenoma (usually benign tumor) that could be causing the problem.
If LH is high but testosterone is low, the issue is testicular, and the cause should be explored.
The HCG Connection
You might have heard of HCG (Human Chorionic Gonadotropin) in the context of TRT. Here's why it's relevant:
HCG is a hormone that's structurally very similar to LH. It can essentially "pretend" to be LH and stimulate the testicles to produce testosterone.
If your brain isn't sending work orders (LH) to your testicles, HCG is like a forged work order that the testicles can't tell apart from the real thing. They get the order and get to work.
This is useful because:
- It can diagnose if your testicles can actually work (secondary vs. primary)
- It can maintain testicular function while on TRT
- It can help preserve fertility on TRT
More on HCG in Chapter 11: Fertility & TRT.
The Clomid Connection
Clomiphene (Clomid) and Enclomiphene work at a different level. They block estrogen receptors in the brain.
Remember how estradiol suppresses LH through negative feedback? These drugs block that suppression.
Imagine the thermostat (hypothalamus) has estrogen goggles on. These goggles make it think the room is warm (enough estrogen/testosterone) even when it's cold.
Clomid knocks those goggles off. Now the thermostat sees the real temperature and cranks up the furnace (tells pituitary to release more LH).
See Chapter 11: Fertility & TRT for the full discussion of Clomid/Enclomiphene - when they work, when they don't, and why most men prefer actual testosterone.
Why TRT Shuts Down Natural Production
Now you can understand why taking exogenous testosterone (TRT) shuts down your natural production:
- You inject/apply testosterone
- Blood testosterone levels rise
- Some testosterone converts to estradiol
- Both high testosterone and estradiol signal to the brain: "We have enough!"
- Hypothalamus reduces GnRH
- Pituitary reduces LH and FSH
- Testicles stop receiving work orders
- Testicles shrink and stop producing testosterone and sperm
This suppression happens with ANY form of TRT - injections, gels, patches, pellets. It's not about how "natural" the testosterone is. Your body can't tell the difference between testosterone you produce and testosterone you inject - it all triggers the same feedback.
This is why TRT is typically a lifelong commitment and why fertility preservation should be discussed before starting.
Quick Recap
- The HPG axis (brain → pituitary → testicles) controls testosterone production
- LH is the signal that tells testicles to make testosterone
- FSH supports sperm production
- Negative feedback keeps the system in balance
- Estradiol is a major feedback signal - excess body fat can disrupt this
- Primary hypogonadism: testicles are the problem (LH high, T low)
- Secondary hypogonadism: brain signal is the problem (LH low, T low)
- TRT shuts down the natural system by mimicking high testosterone/estradiol
- Understanding this helps you understand HCG, Clomid, and fertility impacts
Next up: Testing Your Testosterone - The practical guide to getting your levels tested the right way.